Wait-and-see
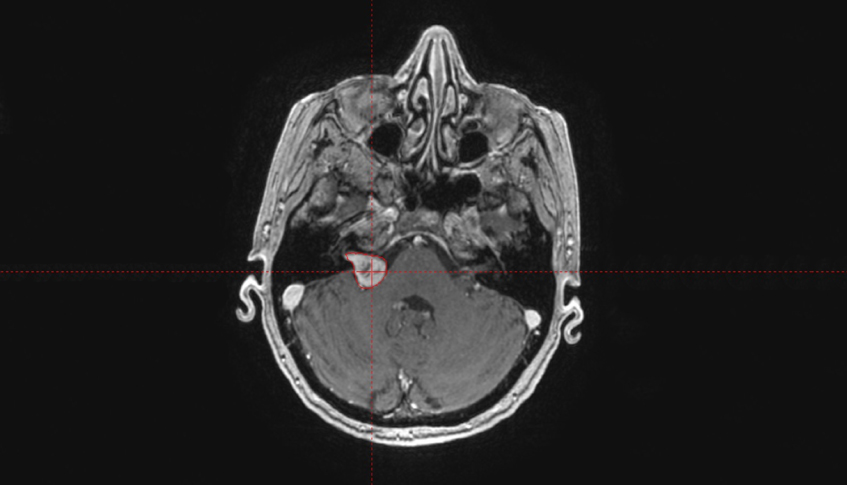
With very small tumors, i.e. less than 1 cm, the spontaneous course can be observed using MRI checkups (wait-and-see). However, you should not wait too long as otherwise permanent hearing damage, i.e. deafness, may occur.
Surgery
Surgery is the primary procedure for large tumors over 2.5–3 cm in diameter. Surgery removes the tumor and eliminates the compression on the brain tissue. The operation is performed under full anesthesia and lasts on average 3–5 hours. Risks primarily consist of hearing impairment through to loss of hearing. In the initial period, significant balance problems and sometimes also facial weakness occur. Serious risks (5%) of this kind of operation include bleeding, secondary bleeding, infection, accumulation of cerebrospinal fluid, or tissue injuries.
Following surgery, the vestibular nerve is destroyed and the patient has balance problems for 2–3 months.
Facial paralysis (facial nerve) is more likely following surgery than following radiosurgery. Permanent facial paralysis may occur with nerve damage.
Radiation therapy
Radiosurgery is an alternative to surgery for smaller acoustic neuromas. Here the tumor is not removed, but killed. Unlike surgery, the skull is not opened. Whether radiosurgery is possible will depend on the size and location of the tumor.